Additional Information On Our COVID-19 Office Updates
To ensure the safety of our staff, patients, and community we have made significant changes to our office to ensure we are providing the safest dental care environment.
In addition to following the CDC Guidance for Dental Settings, we have also decided to follow the CDC Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Although the CDC does not state specifically in the Guidance for Dental Setting that Dental procedures should be performed in Airborne Infection Isolation Rooms (AIIRs), they do state this in the Interim Infection Prevention and Control Recommendations for Healthcare Personnel During the Coronavirus Disease 2019 (COVID-19) Pandemic. Therefore, in order to provide the safest possible environment to perform our care, we have decided to upgrade all of our private operatories to rooms similar to Airborne Infection Isolation Rooms (AIIRs).
We have installed Negative Air Units designed specifically for healthcare facilities. Instead of recirculating the air back into the operatories, air is exhausted outside through metal medical grade HEPA filters as recommended by the CDC. We use the same monitoring devices as healthcare facilities to monitor and ensure the rooms are pressurized correctly. The CDC recommends AIIR rooms be pressurized to at least -0.01” W.C . (water column), we have set our rooms at -0.06” W.C. six times higher than the CDC minimum requirement. Also, the CDC recommends Air changes per hour (ACH) of 12 times for AIIR, each of our rooms are able to produce 50 ACH.
The only difference between our rooms and rooms you would find in a hospital is that our rooms have minor air leakage from wall outlets and ceiling tiles. However, we did perform a smoke test to see if there is visible air leakage between operatories, but were unable to detect any visible smoke leakage. We will post a video of this test and other performance test on our Youtube channel shortly.
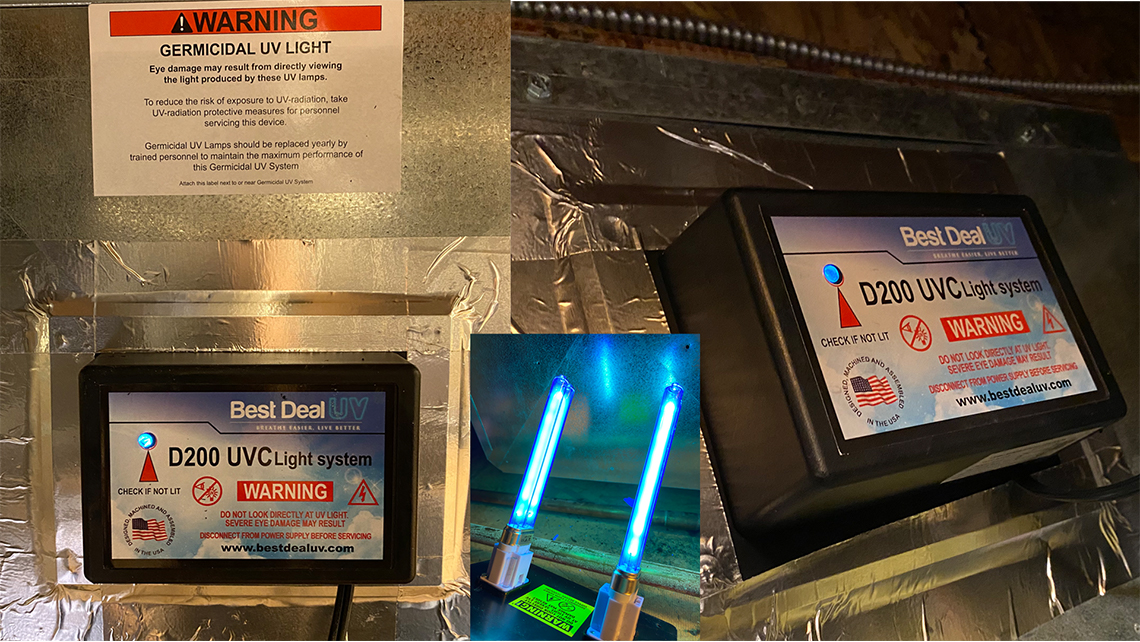
To further disinfect our operatories, we have installed multiple UV-C lights above all of our operatory chairs. We chose to use direct ultraviolet germicidal irradiation because it has been proven to kill many pathogen including SARS-CoV-2 safely and quickly and is recommended by the CDC as a way to decontaminate equipment. Per the CDC, it takes .5 J/cm2 to kill most pathogens. Our lights produce .5/Jcm2 in less than 5 mins at a distance of 7 feet from the floor. The closer to the floor, the long it takes to kill pathogens. To kill 99.9% of pathogens on the floor it would take 30 min with our lights, but because of our high ACH and manual disinfection, we only run our light around 10 mins between appointments. We also run them for 30 mins at lunch and after work.
We also use Kulzer Ivory RELEAF HVE (high volume evacuation) during high AGP (aerosol generating procedures) when 4 handed dentistry is not available. This helps reduce the amount of aerosol generated that leaves the mouth. With helps further reduce the amount of pathogens in the air.
Our reasons we choose not to use HOCL Foggers, LED UVC light wands, portable HEPA air purifiers in our operatories, or Extraoral Dental Suction units. Below are just our own personal opinions based on the information we received from the CDC, ADA, and various other governing bodies. We are not claiming that these solutions do not work or are dangerous; we just decided that they were not a good fit for our office for the reasons below.
HOCL Foggers:
We chose not to use Foggers per previous recommendation by the CDC to not use them in patient-care areas. Although they have retracted it to state “no recommendation/unresolved issue,” we decided that it was still too risky for our staff and patients to use in our office, compounded with the CDC finding that chronic exposure to HLDs like HOCL may cause asthma. Please see CDC links below:
https://www.cdc.gov/infectioncontrol/guidelines/disinfection/index.html
https://www.cdc.gov/niosh/topics/healthcarehsps/disinfect.html
- 2003: “Do not perform disinfectant fogging for routine purposes in patient-care areas. Category IB”
- 2008: “Do not perform disinfectant fogging in patient-care areas. Category II”
- 2011: “More research is required to clarify the effectiveness and reliability of fogging, UV irradiation, and ozone mists to reduce norovirus environmental contamination. (No recommendation/unresolved issue)”
- “Chronic exposure to HLDs may cause asthma and asthma-like symptoms.7,8 Hydrogen peroxide has been shown to be potentially mutagenic in animals.”
LED UV-C:
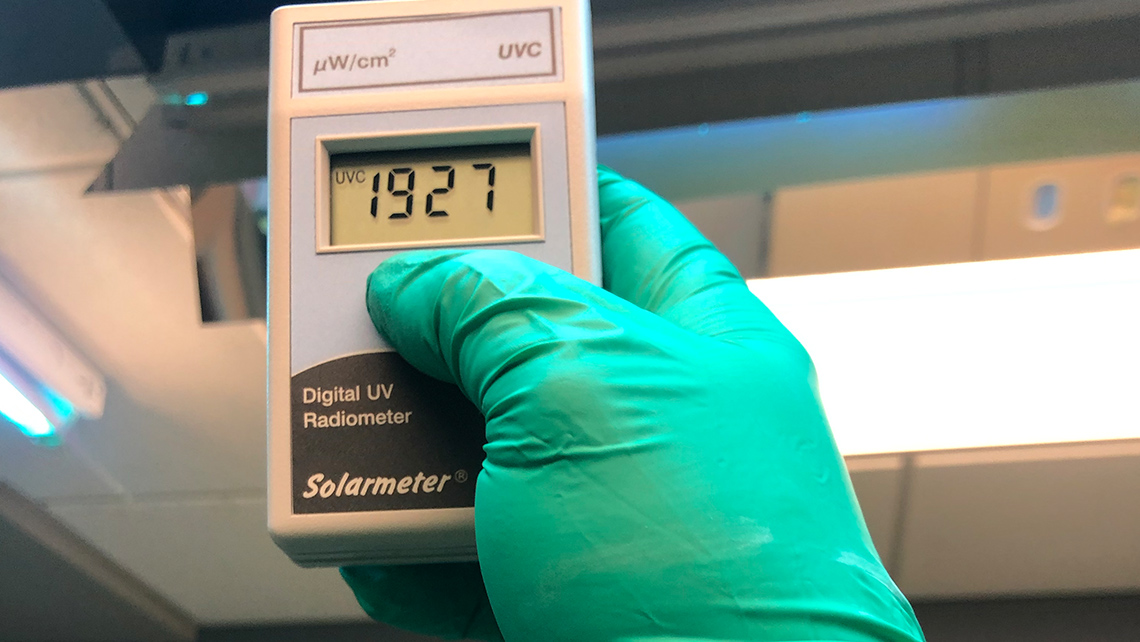
Majority of all LED UV-C lights on the market are fake, and thus, ineffective. We tested a few LED UV-C wands with our UV-C meter and none produced any UV-C rays. Also, if the LED is covered in plastic or anything other than heavy quartz it is likely fake as UV-C can’t penetrate most surfaces including plastic and glass. Here is a link to an article regarding LED UV-C:
https://www.powerelectronictips.com/killing-covid-19-with-uv-c-leds/
Portable HEPA Air Purifiers:
CDC recommends recirculating air through HEPA air filters as a last resort. Most portable HEPA Air filters need to be replaced every 30 days and are only a couple inches thick. Our Negative Air Unit has a metal framed HEPA air filter that is over 12” thick. Portable Air Filters rarely produce over 300 CFM, our unit’s minimum is 600 CFM. Portable Air Purifiers with high CFM ratings are inherently loud and take up a lot of space. We use these portable units only in our common areas where the pathogen loads are not as high and as an adjunct to our HVAC system.
Extraoral Aerosol Suction Units:
Most popular units only have CFM rating of 100 to 300 CFM. The manufacturers also recommend that the suction tip be placed around 1” away from the patient’s mouth, leaving little to any room to perform any procedures. Additionally, these units suffer the same drawbacks as portable air purifiers. They are also loud (around 70db on high settings) and the CDC states that long exposure to noise at 70db can lead to hearing loss.